Key Highlights
- infant mortality rate (IMR)
- Disparity in IMR among States
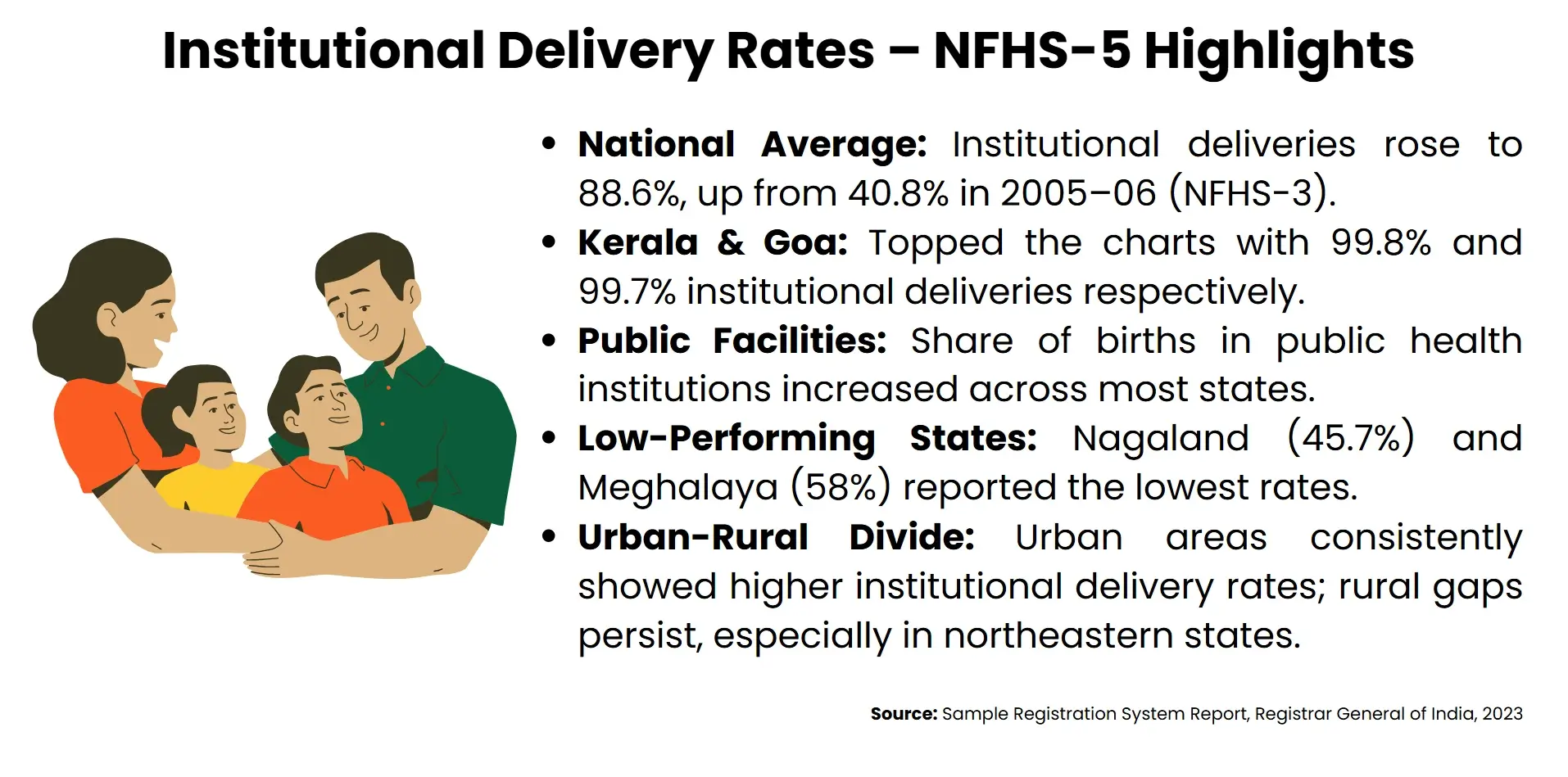
- Institutional Delivery reached 88.6%
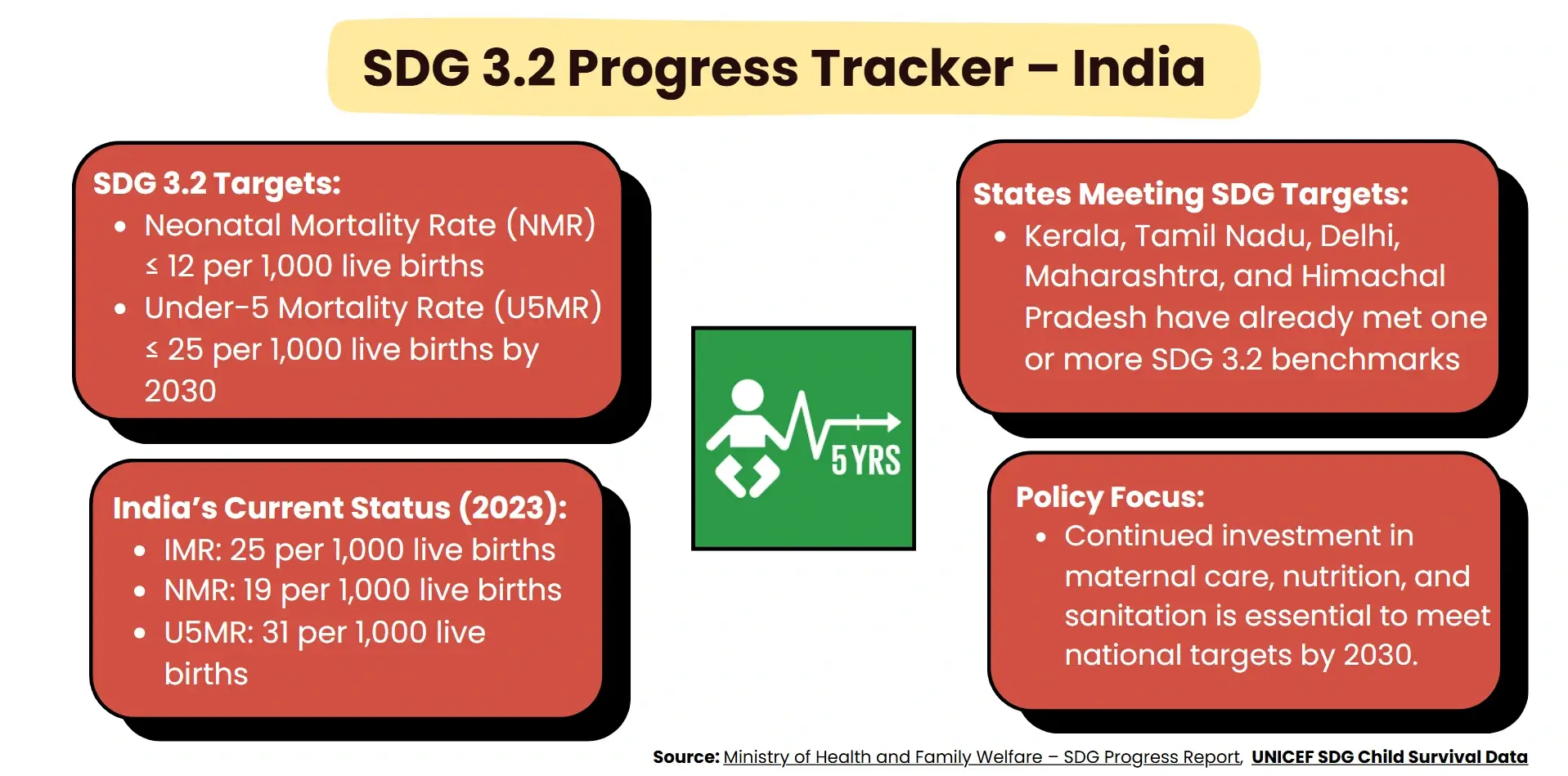
- SDG 3.2 targets for 2030
|
The infant mortality rate in India is at an all-time low of 25 in 2023, and yet, the regional variation is still shocking: the infant death rate in Manipur is 3, whereas MP, UP, and Chhattisgarh have the highest rates, namely 37.

Relevant Suggestionfor UPSC & State PCS Exam
- The IMR in India declined by a significant margin of 37.5%, a key health indicator important for GS Paper II (Governance and Health).
- State disparities in health outcomes are reflected in high-burden states such as Madhya Pradesh, Chhattisgarh, and Uttar Pradesh, which have an IMR of 37.
- The lowest IMR of 3 is in Manipur, and among the most appropriate cases study for ethics and governance paper.
- NFHS-5 reports an 88.6% institutional delivery rate, and Kerala and Goa are near universal coverage.
- SD Goal 3.2: Neonatal mortality≤12 and under 5 mortality≤25 by 2030; in India the current IMR is 25, NMR is 19 and U5MR is 31.
- The importance of policy, equity-based financing, sectoral governance via data and cross-sector collaboration are key in structuring Mains answers.
|
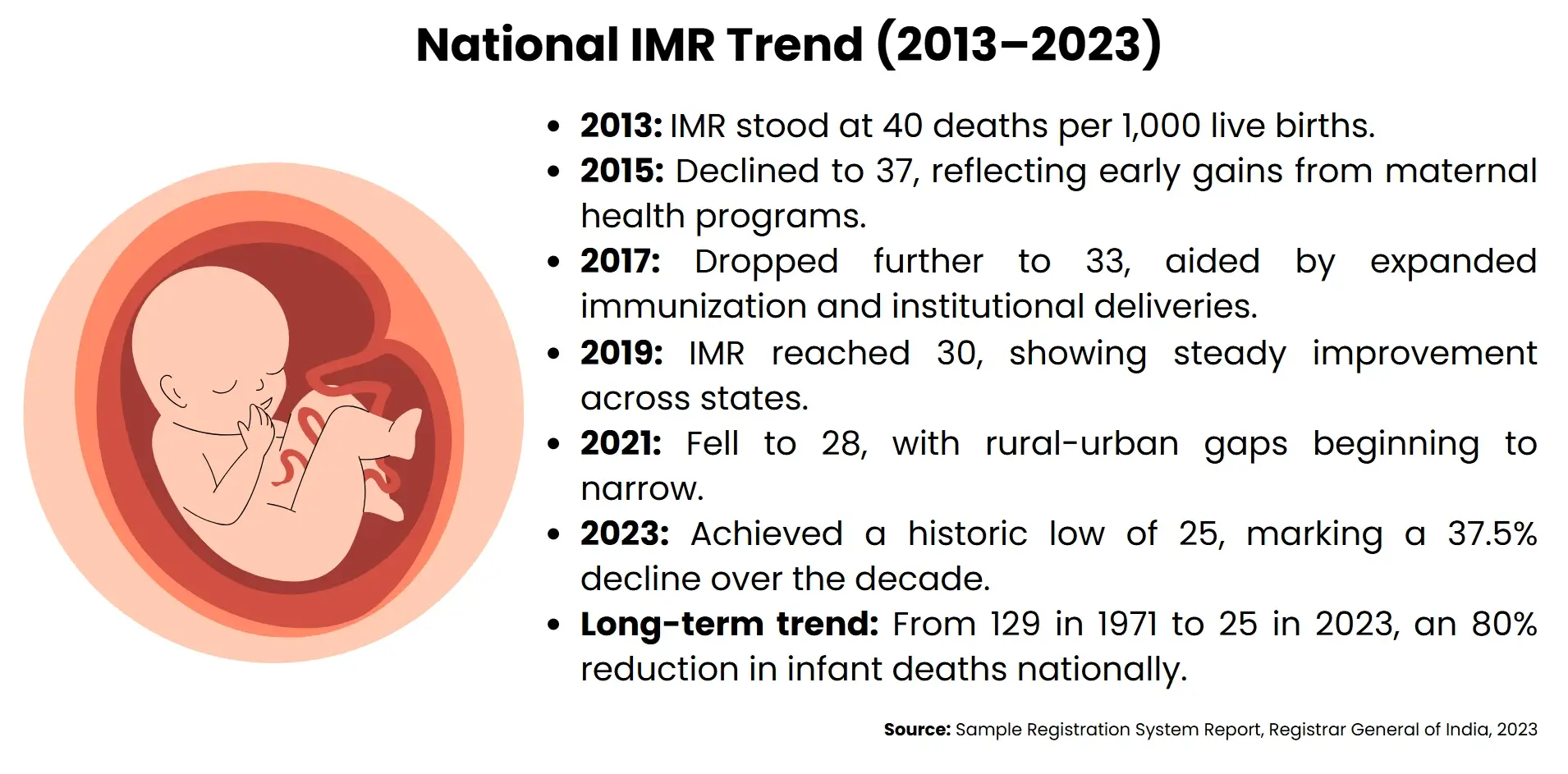
The infant mortality rate (IMR) of India has not been spared either, as it was 40 deaths per 1000 live births in 2013, and according to the latest records of the Sample Registration System (SRS) data, now the death rate is 25 per 1000 live births in 2023. This decline can be considered a significant milestone in the field of public health, as it is the result of a multiplied effect of specific maternal and child health programs, an increase in the number of deliveries at the institution, and an increase in immunization coverage. The national average, though, masks spectacular geographical inequalities that nevertheless raise the question of fairness in health outcomes. States like Madhya Pradesh, Chhattisgarh, and Uttar Pradesh record the highest cases of IMR at 37, which highlights the long-standing failure of healthcare infrastructure, socio-economic development, and service delivery. Instead, Manipur has turned into a success model, with 3 IMR, the lowest in the country, and indicative of what community health systems and inclusive government can do.This article critically evaluates the dynamics of the IMR decline in India, the factors that lead to the differences in the region, and whether the policy responses to the attainment of Sustainable Development Goal (SDG) related to child survival targets have been achieved. The discussion would also base future structures of mainstreaming vulnerable populations, along with strengthening the national responsibility of India by preventing preventable cases of infant mortality through analysis of development gains, as well as confirming that inequalities exist.
India's Infant Mortality Rate Hits Historic Low
In the year 2023, the infant mortality rate (IMR) in India has hit a historic low of 25 per 1,000 live births, marking a decade of transformative progress in maternal and child health outcomes countrywide.
Decadal fall and Historical Context
The cumulative results of the sustainably-focused, durable interventions to promote health are reflected in a positive change of 37.5 percent from 40 in 2013 to 25 in 2023. This development becomes all the more impressive considering a span of 50 years: in 1971, the IMR in India was 129, which is 80 percent lower than it was centuries ago. This trend puts India within the line of countries that have had the best progress in child survival rates despite having a huge population size and gross gaps.
Enhancing Policy Interventions and Health Systems
Most of the fall is credited to the specific national programs like Janani Suraksha Yojana, Janani Shishu Suraksha Karyakram, and Ayushman Bharat. These programs increased institutional delivery, antenatal services, and neonatal services, especially in disadvantaged areas. This was further reinforced with outreach and accountability as the theme of the National Health Mission, community health workers, and decentralized service delivery. Immunization measures such as Mission Indradhanush were also of paramount importance in preventing infant mortality, which could have been avoided.
Rural Urban Convergence and Equity Gains
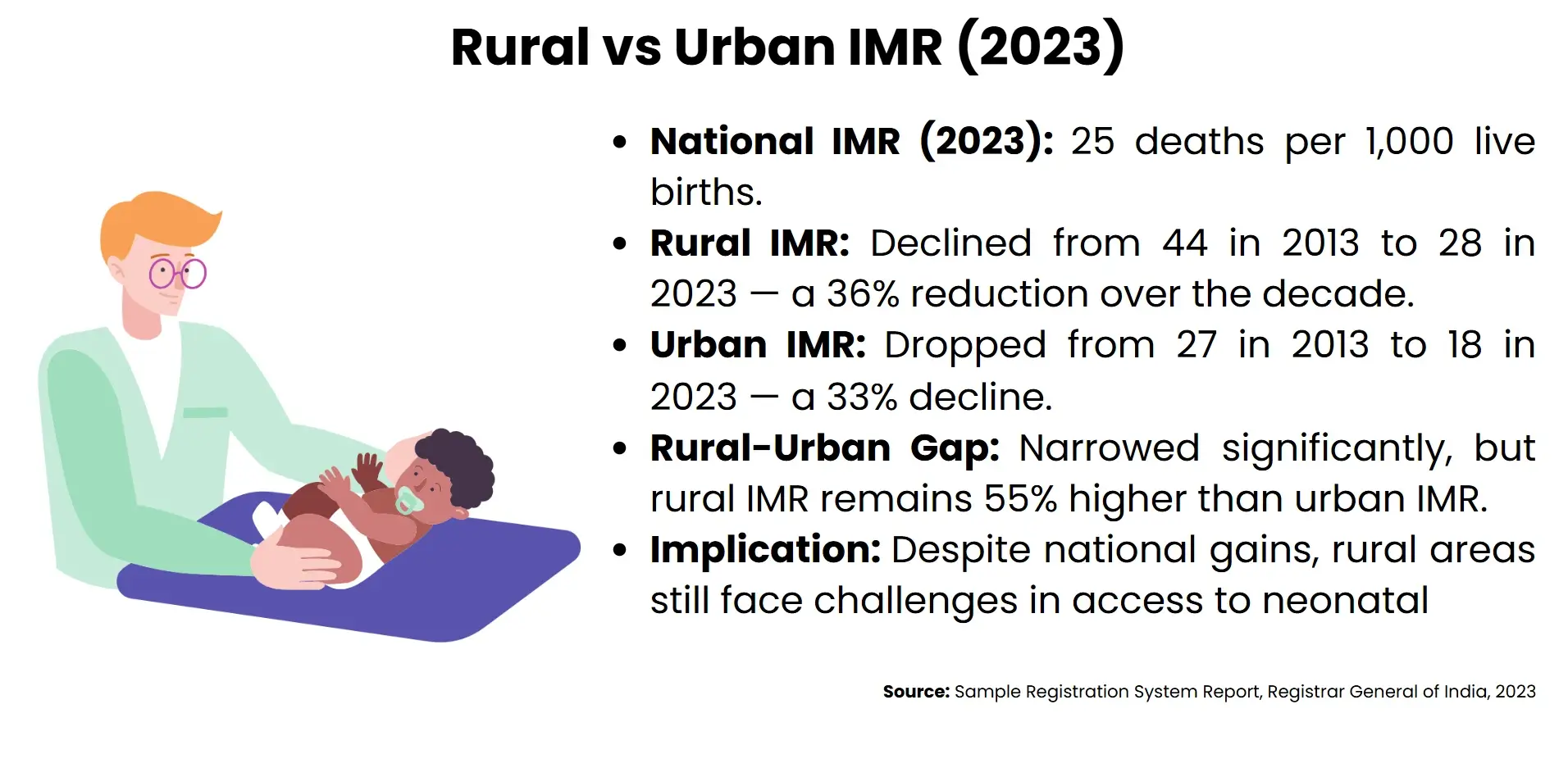
Positively, there is an improvement in the rural-urban gap in IMR. Over the last ten years, rural IMR decreased from 44 to 28, whereas urban IMR decreased from 27 to 18. This convergence can be seen as a sign of better infrastructure, greater health awareness, and greater access to primary care in rural communities. But there is still an imbalance between the states, and to achieve some improvements, even more focused, goal-oriented policies are necessary.
Population and Demographic changes
The demographic situation in India is changing in line with its health indicators. The birth rate in the country decreased over the period between 21.4 in 2013, to 18.4 in 2023, which means that it has reached the maturing population structure. Meanwhile, the mortality rate dropped to 6.4 in 2023 (the usual value is 14.9 in 1971), and it has brought about a general increase in the state of the population. These changes mean that any improvements in IMR would be included as part of a wider population health redefinition, in policy and socio-economic transformation.
Regional Disparities and High-Burden States
The 25 per 1,000 live births national infant mortality rate (IMR) in India is the most recent and illuminates the health disparities ingrained in the local context, where some state zones still record mortality levels that are several times higher.
High-Burden States
The worst affected are Madhya Pradesh, Chhattisgarh, and Uttar Pradesh, which have all recorded a higher IMR of 37 than the national average. These states bear the uneven disproportional rate of infant deaths due to the combined failure to provide healthcare, maternal nutrition, and infant care. The growth of these areas has been slower than in the rest of the country, even given national efforts, suggesting structural impediments (low concentration of the working population in health, broken referral, and inadequate sanitation).
Determinants, Socioeconomic and Infrastructural
The high IMR of these states is highly associated with multidimensional poverty, low literacy levels in women, and the inability to access quality antenatal services. In these areas, rural inhabitants tend to be geographically isolated and lack facilities to adequately address their health needs. In the most straightforward example, Chhattisgarh not only has one of the highest IMRs, but it also has the highest number of deaths per 1,000 people at 8.3. Caste, gender, and economic marginalization all interact to increase the inequities in health, particularly in tribal and remote districts.
Lessons from Low-IMR States
By contrast, Manipur has not only the lowest IMR in the country (only 3) but also the least. This has been possible through strong systems of community health, excellent maternal outreach, and culturally sensitive service provision. Single-digit IMRs are reported in Kerala and Himachal Pradesh, illustrating the effect of years of investment in the infrastructure of a publicly funded health system, female education, and decentralized governments. These states provide examples that could be adopted with the primary care and social determinants of health integration.
Policy Imperatives for Fair progress
The solution to regional inequalities is to move away from nation-wide objectives and use region-based approaches. High-burden states prefer to strengthen the efforts of frontline health workers, elaborate data systems, and provide an accounting service delivery. There is a need to improve intersectoral coordination between health with nutrition, education, and sanitation. Along with this, performance bonuses and concerted funds can be utilized in order to streamline the underperforming districts. In the absence of deliberate efforts, India will experience imbalanced developmental strides towards its Sustainable Development Goals (SDG), especially SDG 3.2 on the ending of preventable deaths of children.
Outstanding performance by Manipur
The success of public health in Manipur is perhaps a story of the highest national figures, yet simultaneously a clear example of a low infant mortality rate (IMR); the Indian State of 3 deaths per 1000 births in 2023 stands out as an example of a successful reproductive and maternal healthcare nationwide.
Health Governance based on the Community
Manipur has a community-based and decentralized approach to the health system. Since its establishment in 1951, the Directorate of Family Welfare Services has been focused on maternal and child health, and incorporated the local governance procedures into the health delivery structures. Early antenatal registration and immunization are ensured at the village level with the assistance of Accredited Social Health Activists (ASHAs) and the auxiliary nurse midwives (ANMs). These are grassroots efforts that have created trust and increased health-seeking behavior, particularly in rural and tribal populations.
Maternal health innovations and institutional delivery
The state has tried several maternal health innovations, including Birth Waiting Homes in remote areas where expectant mothers may seek safe havens in close proximity to health facilities. NFHS-4 to NFHS-5 institutional delivery rates increased to 79.9 per cent, of which more than half of all births (59.1 per cent) were done by a public facility. Efforts such as Janani Shishu Suraksha Karyakram (JSSK) and SUMAN have also reduced the cost burden of care, and mothers and newborn children can be transported, diagnosed, and treated free of charge.
Preventive Care and Immunization
Immunization coverage is one of the most advanced in the country and in Manipur, the goal is to achieve full immunization of babies by 90 percent by the end of 2025. Planned outreach activities in the relief camps and conflict-inflicted areas (planned by the state) have provided continuity in care even during disruption. Iron and folic acid supplements among pregnant women increased to 30.3 percent in comparison to 16.3 percent as a nutritional surveillance and counseling improvement indicator.
Policy indicator Strength
The literacy level (79.2) and sex ratio at birth (967 females per 1000 males) of Manipar support the good maternal and child health indicators. The relatively low level of population and the high level of rural activity allowed the state to use strictly targeted interventions. Its Family Welfare Program is in tandem with Sustainable Development Goal 3.2, which is to curb neonatal mortality and avoidable infant mortality by implementing service delivery and health equity frameworks.
Policy implications and Future directions
The decrease in infant mortality rate (IMR) in India, which is currently 25 per 1,000 live births, reflects one of the biggest public health successes. However, such momentum requires strategic policy recalibration and region-specific interventions in order to be maintained.
Strengthening Health Financing Equity
Even with the development of a nation, there are differences in states that underscore equity-based resource distributions. States in the high burden category, like Madhya Pradesh and Uttar Pradesh, need more budgetary allocation to maternal and neonatal services. Decentralized planning, performance-based incentives, and conditional cash transfer should be scaled so that vulnerable classes, particularly tribal and rural, receive quality and timely service. Local health systems can address the situation with greater effectiveness through the strengthening of fiscal devolution by the National Health Mission.
Data Driven Governance and Monitoring
Strong data systems are needed to track the IMR trends and signal gaps in the service. To improve transparency and accountability, geospatial mapping, health management information system (HMIS), and real real-time dashboard can be introduced. States need to invest in civil registration and vital statistics (CRVS) to have appropriate birth and death reporting. The results of the Ballabgarh project and NFHS equity analyses indicate that interventions targeting the local population and, crucially, based on data, can manage neonatal mortality rates to a significant degree even in socioeconomically deprived areas.
Cooperation between sectors and SDG alignment
Meeting SDG 3.2,ending preventable infant deaths by 2030, means that the sectors need to work together. Child survival strategies should include nutrition, sanitation, education, and gender equity. Mothers' health programs such as POSHAN Abhiyaan and Swachh Bharat should be synchronized with programs aimed at underlying determinants. The examples of effective Holistic governance, cross-sector synergy implementation are provided in the states where the SDGs have been realized, like in Kerala and Himachal Pradesh.
Innovation and Social Responsibility
Such a policy in the future must focus more on service delivery innovation (telemedicine, mobile health units, and AI-assisted diagnostics in rural areas). The community is kept at the center of interest, the last-mile gaps can be bridged by training the ASHAs, empowering the women groups of the area, and building local accountability. The achievements of the community-based maternal care model in Manipur show that culturally responsive systems are capable of providing better outcomes than national averages despite their lack of resources.
Conclusion
The remarkable infant mortality rate decrease to 25 per 1,000 live births in 2023 in India is an impressive indicator of positive changes in the national health delivery and maternal-child care systems. But this national success is moderated by the endemic regional inequalities, with states such as Madhya Pradesh, Chhattisgarh, and Uttar Pradesh still reporting even higher IMR rates. By comparison, the impressive case of Manipur highlights the potential to transform the existing healthcare system through community-based health governance and focused maternal outreach. Such inequalities of result are those that indicate the immediate need to promote equitable forward progress using equity-based policy frames, improved informational infrastructure, and trans-sectoral coordination. In applying to the future plans of India to take planning of vulnerable groups into consideration, increased responsibility, and be innovative towards service delivery, given the current progress of the country towards meeting its Sustainable Development Goals commitments, especially that of SDG 3.2. The way ahead is not to maintain national gains but also to bridge sub-national divides so that all children, despite geography or circumstances, have equal opportunities not just to survive but thrive.