India's public health governance is characterized by a complex, fragmented structure with responsibilities spread across various levels of government, leading to coordination challenges. It is critical that the recent growth of doorstep health services in India is supported with a matching growth in civic engagement to co-design, monitor and govern health systems to build equity and resilience.

Health and Wellness Centres and mobile medical units are deployed with an ambitious scheme to make a transformative change in public health service delivery and fill longstanding gaps in access and equity, as well as community engagement. But success is not only infrastructure and logistics dependent, but also the active participation by the populations concerned.The present article focuses on how the key role civic engagement plays in enhancing India's health governance. It suggests that meaningful involvement, such as local monitoring and co-design of services, makes accountability, responsiveness, and resilience possible. Relying on case studies drawn throughout India, this article underscores how the community-based efforts, use of digital technologies and participatory models of governance make passive beneficiaries active stakeholders. Additionally, it highlights the need to have a change of policies, which is the institutionalization of participatory mechanisms to ensure that the health systems are efficient and also fair.Last but not least, the article aims to change the paradigm by switching from top-down service delivery to bottom-up health democracy. In this manner, it points to an attractive future with more just, inclusive, and sustainable public health.
Why Civic Engagement Is Non‑Negotiable in Health
Engagement and civic engagement an aspects of modern health that cannot be lost. The best results concerning better design and governance of health systems are attained when the communities are actively involved in the process of planning, design, and management of health systems. The heterogeneity of India's socio-cultural environment points to the failure of purely top-down responses, especially those in marginalised areas, where such an approach tends to miss localised demands. Where this inequity exists, civic participation addresses the balance by enabling the expression of needs, the co-designing of solutions, and the tools to build accountability that a healthy ecology of health requires.
Participating citizens act as monitors, partners and innovators. The role they play is monitoring service-delivery and managing resource-allocation, and modifying interventions to localised realities. An example is community health committees and participatory audit, where they have improved maternal care and sanitation in a number of states. Additionally, civic engagement reinforces inter-social allegiance that is a critical factor towards preventive care, immunisation campaigns and behaviour-change programmes.
The shift toward digital health and decentralised governance implies a simultaneous change in the role of civil participation. Mechanisms of consultation to influence budgets, data to inform policies, and assess consequences need to be institutionalised. Without such mechanisms, health systems may become technocratic silos that have lost contact with the populations that they are meant to serve.
Ultimately, civic participation is neither a democratic ideal nor a dreamy aspiration rather it is a reality of realism. In converting the docile recipients into active guardians of the public health, it ensures that care not only flows into the communities, but that it is also the property of the communities on which this care depends.
The Current Gaps to fix
Although India has made tremendous strides in the scaling of doorstep health services, there are still some gaps in the system that serve to stifle its performance.
- Imbalance in service provisions and community needs: Commonly used public health interventions are standardized and do not take into consideration the local situations, such as cultural practices, language disparity, and geographical limitations. The absence of this oversight leads to failure in exploitation and creates suspicion, especially in the tribal and remote areas.
- Toothless accountability structures: Most frontline employees are working with little or no proper supervision and feedback mechanisms. Also,grievance redressal systems are not in place or are inaccessible. In the absence of transparency in monitoring, inefficiencies and equity failures.
- Little use and adoption of digital health tools: Digital solutions hold exciting potential in terms of accessibility, but the use and integration of them is not evenly distributed or well integrated. Sometimes, vulnerable groups cannot reap their full benefit due to low digital literacy, uneven internet networks, and a lack of multilingual platforms. Also, the data-gathering in the process is often done without community permission and incorporation, and it does not provide actionable information.
- Empowered, symbolic civic engagement: The existence of health committees and the local forums can be taken as a sign of a symbolic, but not empowered, community involvement. Such a command-line model blocks innovation and responsiveness.
India needs to go all the way to democratizing health systems, which entails broadening the design process, strengthening accountability and the empowerment of civic spaces. It is critical not only to close these gaps to ensure the efficiency of the services provided but also to develop trust, resilience, and long-term health equity.
Ladder of Participation
Ladders of Participation is a conceptual framework that goes further than business-as-usual delivery of services to imagine a dynamic system whereby citizens participate as decision-making entities at all levels of care. At the bottom of the ladder, there is the awareness that is to make sure that people know their rights and what services they can receive. As ascendancy increases, engagement becomes more advanced at the community health forums, where one can give feedback regarding service quality and accessibility and eventually influence program planning and policy.
In the middle of the ladder, communities take on the co-design roles by developing the outreach approaches, designing specific health education, and recommending culturally competent models of service delivery. Citizens, at the upper levels, take up the roles of governance, over-sighting budgets, judging results and making policy decisions. This gradual involvement brings change in the health systems replacing the bureaucratic system with a people-driven ecosystem.
And such a continuum also meshes with life-stage care that ismaternal health to elder support, such that engagement changes as the needs of the population change. The inclusion of the younger and older generations may look like, for example, digital health campaigns being led by youth and elders leading practices in traditional wellness.
Through the institutionalization of this ladder, India will be able to develop a sense of trust, responsibility, and creativity. It is not just a paradigm of consultation; it facilitates co-ownership. As communities go up the ladder, care is not only rendered to them but it is defined, maintained and kept to reflect their lived realities, hence defining the fundamental principles of the participatory health democracy.
Eight mechanisms States can deploy
In this environment, eight mechanisms are suggested to help to incorporate civic engagement into the Doorstep Health Revolution in India. Instead of depending on symbolic interpretation, states are expected to integrate scalable systems in accordance with making the community shareholders of the governance of public health.
PHNAs: Participatory Health Needs Assessments
Gram Sabha, the ward committees and the frontline workers should start bottom-up planning to map out the local health priorities such as the disease burdens, seasonal risks and social determinants. They include transect walks, community surveys and participatory rural appraisals (PRAs), which access lived realities that are usually excluded in top-down data. Deep ties to the local context through ownership anchors interventions, and make them relevant.
Block and Ward Level Co-Design Labs
The establishment of time-boundco-design labs can enable group prototyping between citizens, health workers, and administratorse.g. during the route planning of the mobile-clinic or customization of health-education materials. The labs will have the capability to meet once a month at block headquarters or urban wards and they can be piloted with small funds. The district health orders facilitate the scaling of promising initiatives and, in so doing, promote innovation that is based on community insights.
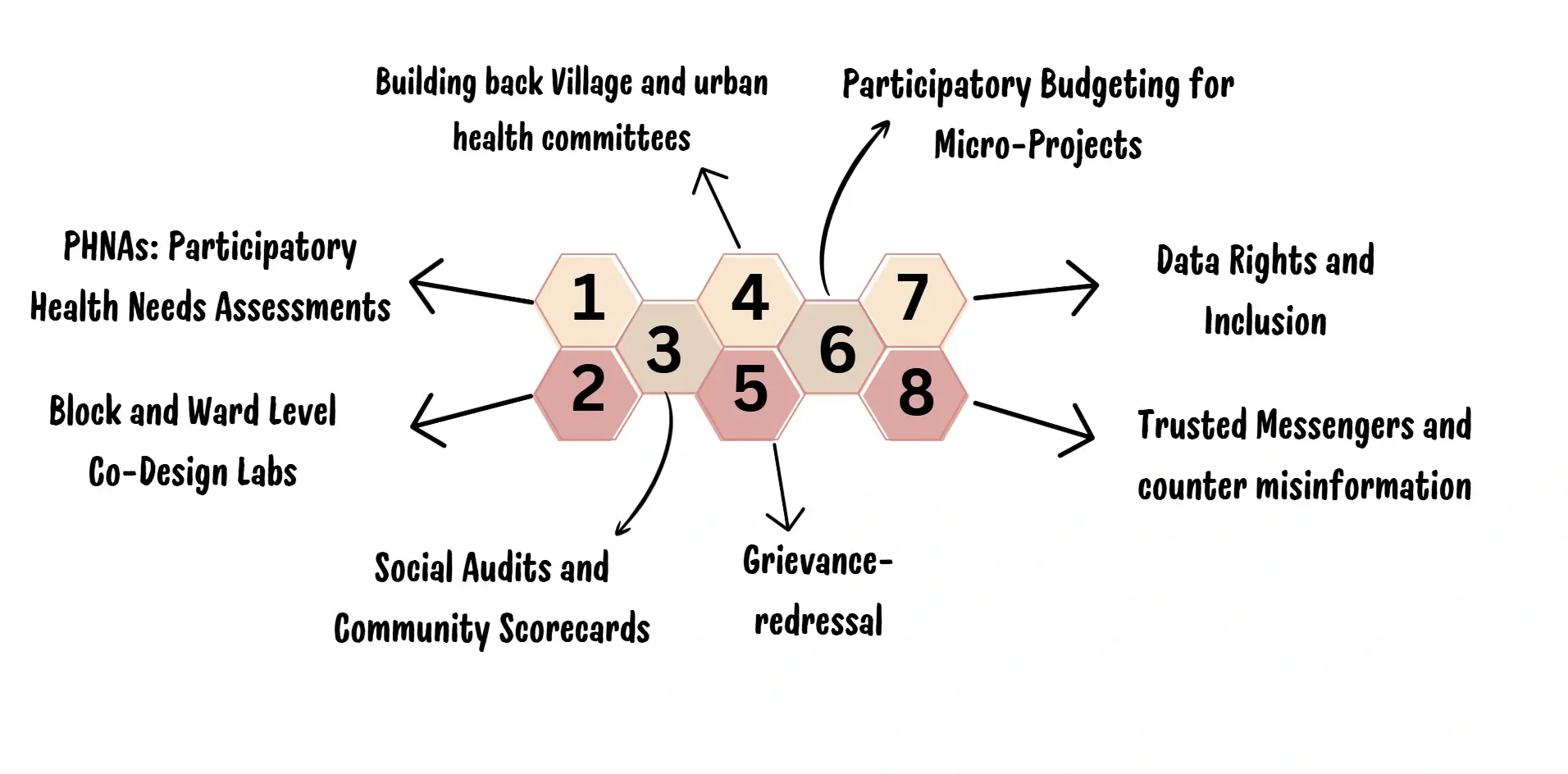
Social Audits and Community Scorecards
It is important to institutionalize quarterly scorecards to assess the availability of services at Health and Wellness Centres, mobile units, and telemedicine services to enable the local users to grade the availability of services, staff behaviour, medicine stocks and wait time. Transparency and accountability are created by visible spread of results on noticeboards and digital dashboards. Independent observers can bring about social audits, which help to connect the results of the auditing with corrective actions and plans to improve the facility.
WHO, or World Health Organization
The primary responsibility of the World Health Organization (WHO), a specialized body within the United Nations system, is to address global health issues. WHO was founded on April 7, 1948, and is headquartered in Geneva, Switzerland. Its mission is to promote global health for all future generations.
Building back Village and urban health committees
City ward health committees and Village Health Sanitation and Nutrition Committees (VHSNCs) should be reactivated with explicit mandates, operating bylaws and un-tied funds. To avoid elite capture, states ought to ensure that meetings be held once a month, in quorum, with formal minutes and rotation in the leadership. The capacity and legitimation development requires training of committee chairs and secretaries.
Grievance-redressal
Governmental accountability is in direct proportion to grievance-redressal mechanisms. In this regard, ideal designs must consider the disease-relevant helplines, WhatsApp, interactive-voice-response systems, and walk-in periods at the ward levels. The management of complaint must become digitalized in order to capture indicators of the time-to-resolution, but unresolved cases must be driven to district health societies in systematic manner. Monthly publication of grievance dashboardscanwork as the trust mechanism for the people.
Participatory Budgeting for Micro-Projects
States can guarantee fiscal accountability, with budgetary contributions of 1-2 % of health budgets divided up in community-prioritised micro-project proposals, i.e., shaded waiting places, transport vouchers, or water points. The first and foremost is transparency that incorporates projects to be voted on by the citizens, work plans put on display, and the receipts, selective photographs and detailed expenditure reports should be accessible to people. Such actions establish that the low budget and high-impact functions are funded.
Data Rights and Inclusion
Digital-health data governance is a controversial issue. The platforms are obliged to protect the informed consent, offer multilingual support and meet the requirement of being offline-first compliant. Data stewards should be assigned to the community to detail to the community use of data and privacy. Stakeholder trust can be enhanced by such public documents documenting the positivity of data use in outcomes such as enhanced referrals to medicine stocking among others. Opt-out mechanisms and the lowest levels of data collection must be heavily implemented.
Trusted Messengers and counter misinformation
Counter-measures that fight misinformation are essential. States are advised to prepare ASHAs, teachers, youth figures and religious leaders as credible health ambassadors to pre-bunk rumours using relatable stories and vernacular. WhatsApp groups, mohalla meetings, and community radio are helpful for disseminating accurate information.

Risks
The health reforms anchored in the government-centered initiatives are especially prone to the deficiencies at the systemic and working level. The risk of elite capture also stands out as one of the major risks in most settings as the dominance of influential individuals in the local health committees marginalizes the vulnerable populations. In addition, digital exclusion, which is reflected in the isolation of communities with a low level of literacy or poor access to the Internet, is another threat, since sometimes even technology-based platforms can remain out of reach. Equally, any abuse of peace-time health information such as unauthorized sharing or profiling, is liable to undermine the trust by the people. Another effect of heated pilots and ambiguous mandates can be the emergence of administrative fatigue due to administrative fragmentation. The cooperation can be also weakened and the distrust is develop through misinformation, especially in the case of a health emergency.
Mitigation Strategies
States ought to employ a leadership through rotation system, gender quotas and promotions of transparent meeting guidelines to curb elite capture. Digital connections beyond digital divides entail the online-offline tools, interfaces that support multi-linguality, and community digital stewards. Data governance requires the chief characteristics of informed consent, data collection minimization, and accountability dashboards to be made accessible to the people. Due to integrated planning, interdepartmental coordination, and mid-year review, fragmentation can be avoided. To fight the misinformation, trusted messengers, hyper-local media, and pre-bunking is needed.
Conclusion
The health transformation of India is more about infrastructure and innovation as well as incorporating a community voice on all levels of governance. The measures to be covered here offer states a viable, time-limited plan to develop inclusive, accountable, and resilient health systems. Anticipating threats to reforms, including elite capture, information asymmetries, lack of transparency, digital exclusion among others, health departmentsneeds to implement specific mitigations to make reform efficient and ethical. The civic activities must shift toward enacting organized co-governance as opposed to ritual consultation, whereby citizens are able to set agendas, oversee performance, and protect information. Co-creation is when communities are part of the development of health systems; when this happens, not only do communities trust each other more, and gain better results, but equity becomes the reality that it is our goal instead of a dream. The broad task is to make care democratic; the coming decade in public health should be shaped by involvement, by accountability and by a sense of mutual obligation, and India can build on the doorstep health revolution and make this the paradigm of participation as well as inclusive government.